

IOP vs. Inpatient vs. Outpatient: Which Level of Care Do You Need?
Do you feel like standing at a fork? Not a dramatic one with storm clouds or theatrical lighting. Just a quiet moment of reckoning, the kind that arrives after enough difficult weeks have accumulated into something unexplainable. You know you need help. That part is settled. What kind? You don’t know yet.
Two roads open in front of you. One is familiar with the weekly appointment. The fifty-minute hour and the same office every week. Then comes the unfamiliar, which is a little frightening. An admission, a facility, the full surrender of your regular life.
There is a third road, less clearly marked, that runs between them. IOP. It is where a significant portion of people who need treatment in fact belong. Programs built for the space where most struggles genuinely live, somewhere between managing and crisis. To find your path, you must understand the three roads, who they serve, and how they differ.
Outpatient: The Foundation, and Its Honest Limits
Standard outpatient therapy is where most people begin, and for a meaningful portion of them, it is exactly right.
The structure includes a scheduled session, typically fifty minutes, once or twice a week. Therapists familiarize themselves with your specific needs over time. The entire space is designed for reflection, for working through the specific, the personal, and the historical. There is real and documented value here.
The honest limitation is arithmetic. One or two hours per week means the other hundred and sixty-six are unstructured. For someone with mild to moderate symptoms, having a stable home environment and a supportive system makes that ratio workable. The session offers orientation, while the surrounding life offers sufficient stability to apply the learned concepts.
However, for someone whose symptoms are actively interfering with daily functioning, weekly therapy cannot keep pace with what is happening. The gap between sessions is not neutral time. It is where the problem lives and operates, largely unchecked.
Standard outpatient therapy asks an implicit question: can your life hold you between sessions? If the answer has started to become uncertain, the next level of care exists for precisely that uncertainty.
Inpatient: When the Environment Itself Must Change
Inpatient care is a different category of intervention, built for a different kind of clinical reality.
Inpatient care lessens the risk to a person’s safety by taking them out of a dangerous environment in cases where it is not possible to keep them in an uncontrolled environment. Round-the-clock supervision. A multidisciplinary team is always on the lookout to monitor stability. No journey back home at the end of the day since home is not where they should be right now.
The average inpatient stay runs three to seven days, and that brevity is deliberate. Inpatient’s clinical goal is stabilization, not the long work of recovery. It contains the acute crisis, regulates medication, and manages immediate safety. Then it transfers the person to a step-down level of care, typically PHP, where recovery can actually be built.
PHP is a level of care that bridges inpatient and intensive outpatient services, designed to facilitate this transition without the disruption of full hospitalization. The structure is substantial: five to six hours per day, five days a week, typically running from morning through early afternoon. Medicare defines the threshold at a minimum of twenty hours of therapeutic services per week.
PHP is appropriate for the person who may be stepping down from inpatient and not yet ready for less structure.
IOP: Where Recovery Gets Built Inside the Real World
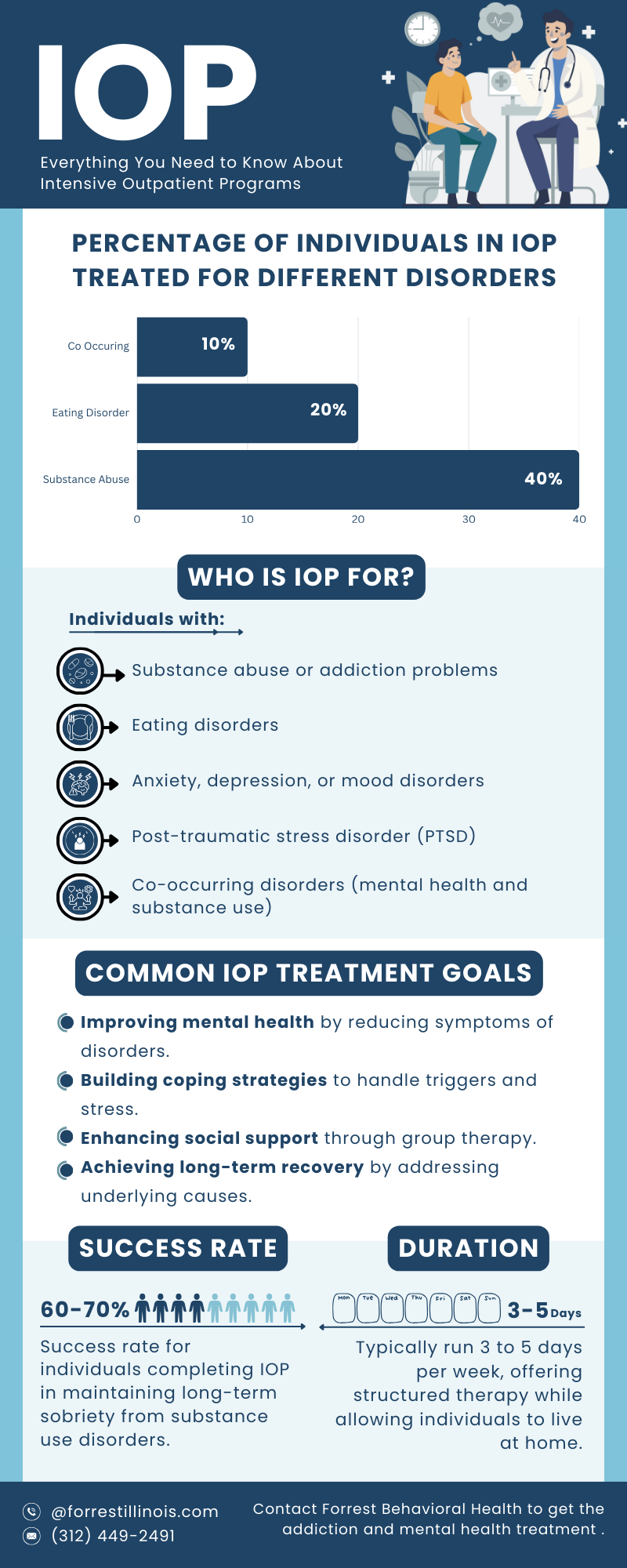
An Intensive Outpatient Program does not ask a person to leave their life. It asks them to bring their lives into treatment and then return to test what they’ve learned.
The format: three to five sessions a week, usually three hours a session, with a total of nine to fifteen hours of programming each week. The central part is made up of group therapy, as well as individual counseling, psychoeducation, and skills training.
Work remains possible. Children still need to be picked up from school. The apartment is still the apartment. The only aspect that changes is the density of clinical support and the frequency with which skills are practiced and reinforced.
The best part is that the skills do not change to become theoretical. They get tested in real conditions, in real time, inside the everyday life the person is trying to repair. IOP research suggests this is precisely what gives the model its durability: recovery built inside ordinary life tends to hold inside ordinary life.
The peer group is a clinical asset that deserves more acknowledgment than it typically receives. In IOP group therapy, people discover that their thought patterns, avoidance strategies, and internal logic around use or self-harm are not uniquely their own.
IOP is the right road for the person who is symptomatic but stable. The one who has not reached crisis, has somewhere safe to sleep, and can manage basic daily responsibilities, but who needs significantly more than a weekly appointment to build traction in recovery.
Final Words
The person standing at the fork rarely has enough information to choose correctly on their own. Distress distorts the assessment. Depression argues that nothing will work. Anxiety argues that any choice could be catastrophic. The brain area most affected by a person’s experience is also the one asked to assess its severity.
A clinical assessment resolves this. It asks not how you feel about your situation but what it actually looks like. Symptom severity, functional impairment, safety, support system, and history. It produces a recommendation grounded in something more reliable than the distorted self-perception that suffering tends to generate.
Rhode Island Behavioral Health offers a range of programs that cover this entire spectrum. If you’re at the crossroads and unsure which road is yours, that uncertainty is not an obstacle. It is the beginning of the conversation.
You do not need to arrive with certainty. You need to make one call. Reach Forrest Behavioral Health at (312) 449-2491, or verify your insurance directly on their website before your first conversation.









