

What A Day In A PHP Program Looks Like (Full Breakdown)
You have already calculated the situation. Weekly therapy? One hour, every Tuesday, maybe every other Tuesday, is not keeping pace with what is happening inside you. The days between sessions are long, and you are managing them in ways you would rather not examine too closely.
Inpatient feels like a different category of problem. The kind that happens to other people, in more visible crises. You are functional. Difficult, but functional. And so you stay in the middle: not well enough to be fine, not broken enough to justify the more serious interventions.
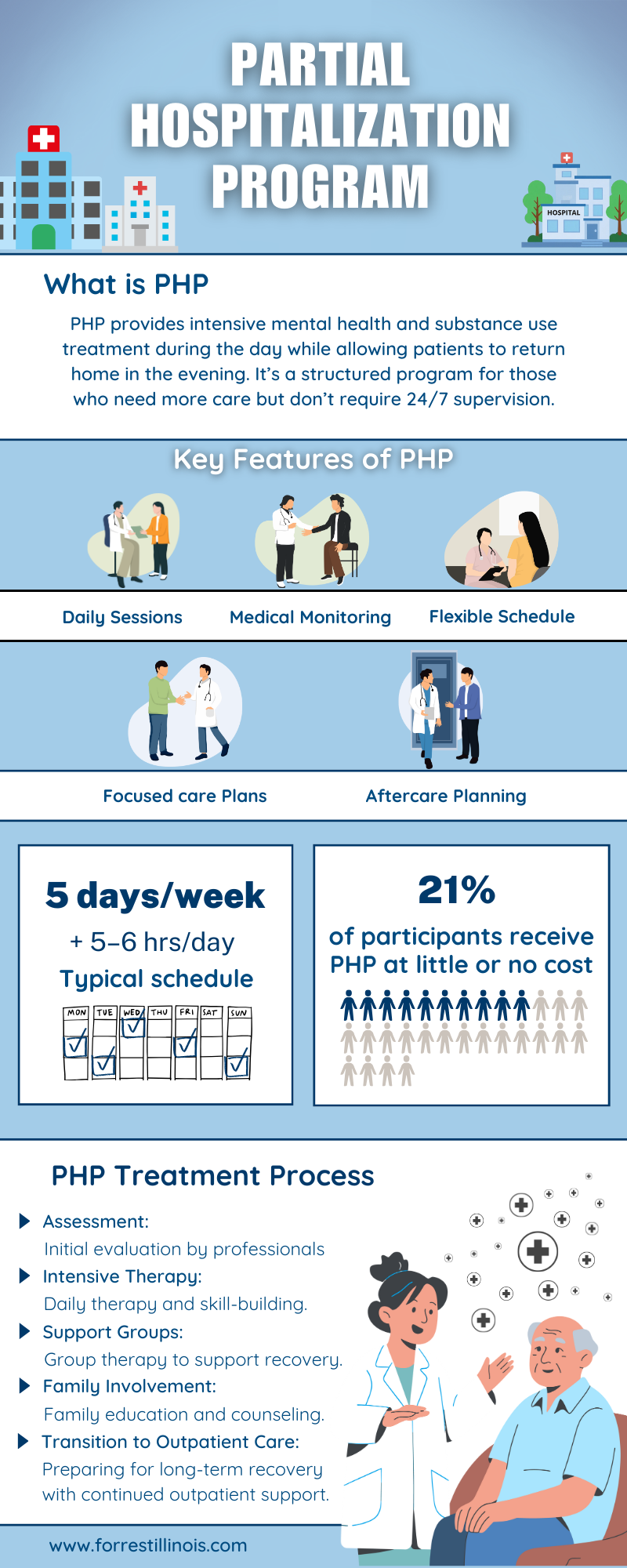
That middle place has a name. A Partial Hospitalization Program exists precisely there, in the gap between outpatient and inpatient care. It was designed not as a compromise but as a specific answer to a specific kind of struggle. What follows is what a day inside one actually looks like. Not the brochure version, but the human one.
Before You Walk Into The Program
The day before your first day matters.
A quality PHP does not begin with a clipboard and a waiting room. It begins with a clinical assessment. A real one that is long enough to address not only the presenting symptoms but also the underlying architecture. The co-occurring anxiety. The sleep that stopped working. The history that keeps showing up uninvited.
Next comes an individualized treatment plan. This is not a standard template with your name typed at the top. Rather, you are given a blueprint that reflects what is going on with you, specifically.
This matters more than it sounds. There is something that shifts when a program demonstrates – before treatment has even begun – that it intends to treat the actual person.
The relief of being accurately seen is itself therapeutic. Some people feel it for the first time at intake.
Morning: Structure as Medicine
The day begins around nine o’clock.
There is a morning check-in, and in programs that do this task well, it is not a formality. It is calibration. A structured group session orients the day by discussing how participants arrived, what they are carrying, and what they are working toward.
The clinical decision to begin with community rather than isolation is not incidental. The distressed brain, the one that has been running on cortisol and avoidance, does not stabilize in private. It stabilizes in the presence of others who are further along than they were last week.
This is the first scaffold. For people who have been struggling alone for months or even years? Being in a room where their internal landscape is recognized can disorient them in the best possible way.
Structure, it turns out, is not the opposite of healing. For a significant number of people in acute distress, it is the condition that makes healing possible at all.
Midday: Time For The Real Work
This is where the day earns its intensity.
Individual therapy sessions place the work in private: the specific, the personal, and the things that do not belong in a group setting. A licensed therapist who knows the treatment plan, has read the assessment, and is tracking the past few weeks.
Group sessions are also conducted in parallel with the therapy, based on evidence-based modalities.
Cognitive Behavioral Therapy operates on the loop between thinking, feeling, and acting, breaking the automatic interpretations that occur before reason can intervene. It rejects the reflexive conclusions that everything worse is permanent; hence, there is no point to living. CBT does not ask a person to think positively. It asks them to think accurately and then provides a skill for doing so.
Dialectical Behavior Therapy adds what CBT alone sometimes cannot reach: the capacity to tolerate what is happening right now without worsening it. Distress tolerance, emotion regulation, interpersonal effectiveness, and mindfulness aren’t mere wellness concepts but clinical tools, practiced until they become available under pressure.
Afternoon: Where Theory Meets the Real
Holistic and experiential therapies enter the schedule. These approaches reach parts of the nervous system that conversation does not always access.
Psychiatric evaluation and medication management are integral to the clinical picture, not an afterthought. When medication is part of the plan, it is evaluated in the context of everything else, not siloed into a separate ten-minute appointment somewhere across town.
Skills practice continues. Distress tolerance rehearsed in a safe environment in the afternoon is more likely to be available at eleven o’clock at night when it is needed. This is not theory. It’s training, and the logic is the same as any other: low-stakes repetition makes high-stakes skills retrievable.
The program is instilling something in a person that they must take home at the end of the day. In the afternoon, they often feel the weight of it and realize they can.
Five O’Clock: Going Home Is Part of the Program
At the end of the day, around four or five o’clock, the person goes home. Same neighborhood. Same apartment. Same relationships with their complicated histories and same pressures that were there before treatment began. The same Thursday evening that used to feel like open water.
This is not a design flaw. It is the point.
A residential program wraps a person in a controlled environment and asks them to get better inside it. A PHP encourages them to improve their everyday lives, which are more challenging and honest. The laboratory and the real world are the same place, and recovery has to function inside both.
Going home is part of the program because that is where the problem lives. Meeting it there, with new tools, the same day they were acquired, is what makes the learning stick.
Final Words
If you searched for what a PHP day looks like, you were probably not conducting research.
You were trying to answer something more personal: Whether the structure would hold you or confine you. It is unclear whether the people inside would understand your specific situation or simply hand you a pamphlet.
Those are reasonable things to want to know before walking through a door. Forrest Behavioral Health’s PHP is built for the person who is not in crisis by the clinical definition, but who is close enough to know they cannot keep managing this alone. The assessment is real. The treatment plan is yours. The day is structured because structure, for a certain kind of suffering, is not a burden. It is relief.
If you think it might be time, reach out. The conversation is the first step, and it does not require certainty to begin.









